
His Patients Once Planned Their Funerals. Now They Plan Their Retirement.
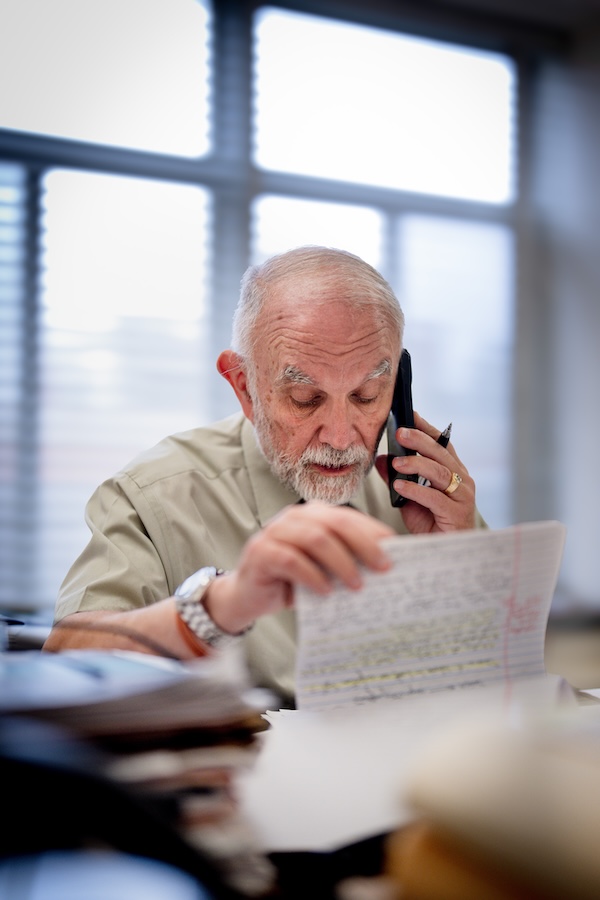
Early in Dr. Peter Gulick’s career, he would find food trays outside of his patients rooms.
Gulick, now 76, was the Lansing area’s leading expert on AIDS/HIV when the condition first surfaced and he remembers hospital staff members were so afraid to enter AIDS patients’ rooms, he would be left to bring their food inside. From the time the mysterious illness was first recognized, he has stayed with patients through the fear, the misconceptions and the lives cut tragically short.
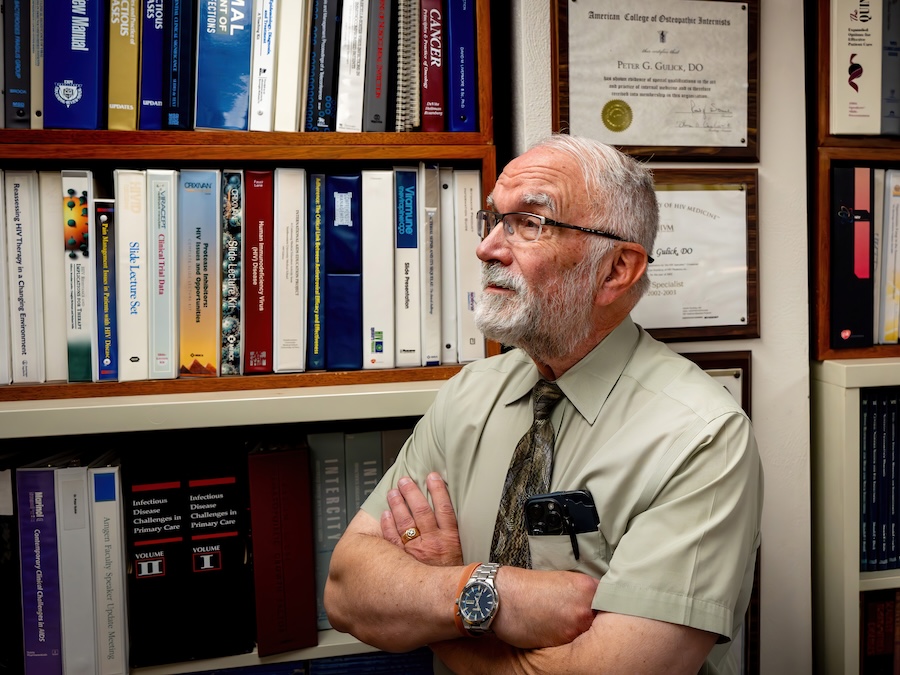
Still on the forefront of the fight against HIV/AIDS, Gulick helped usher in a new era of hope for people living with a condition that was once a death sentence. He wants to continue his work until a cure is found.
Gulick hails from Ohio and attended medical school in Chicago. It was there that he became interested in oncology and understanding how cells become cancerous. He accepted an oncology fellowship in New York, but the distance proved too difficult for his young family. He returned to Cleveland and completed a residency in infectious diseases.
During his training in Cleveland, he saw his first cases of gay men with unusual infections, illnesses that normally affected the very old or were associated with cats and birds.
“Nobody could figure out why a person that was healthy, that didn’t have underlying cancer or anything immunosuppressive, would get these opportunistic infections,” Gulick said.
In 1982, these patients were diagnosed with Gay-Related Immune Deficiency Syndrome, or GRID.
Two years later, Gulick arrived in the Lansing area to take a job at Sparrow Hospital. He was drawn to the area because he enjoyed teaching medical students in Cleveland and could continue teaching at Michigan State University’s College of Osteopathic Medicine.
Because he was a newcomer and had firsthand experience with GRID, or AIDS (Acquired Immune Deficiency Syndrome) as it became known in 1982, Gulick said those cases were assigned to him.
“Nobody else wanted to take care of [AIDS],” Gulick said. “They were all afraid of it. They were afraid of transmission, they were afraid of what it caused, they knew it was devastating if you did catch it. So I was kind of the elected guy with the training that I had, and I started seeing cases when I first got to town.”
Gulick started a clinic through Ingham Medical Center, now McLaren Greater Lansing, where he exclusively treated AIDS patients. There was no effective treatment in those early years, he said. All he could do was identify people who were HIV-positive and examine them. There was still no way to measure outcomes beyond tracking T-cell counts.
If a patient had a T-cell count below 200, he knew that person was at high risk for opportunistic infections that often led to death.
“We just kind of waited for the inevitable to happen,” he said. “We just put out fires. We didn’t really solve anything.”
Gulick learned he could prescribe antibiotics to try to prevent opportunistic infections such as pneumocystis, but doing so could create a different infection, such as cytomegalovirus.
“These were very difficult years,” he said. “I had no support from the community, from the basic community in general, and from the medical community as well because everybody was fearful of what this virus could do. Nobody wanted to take care of patients, so I was kind of left alone to try to manage them.”
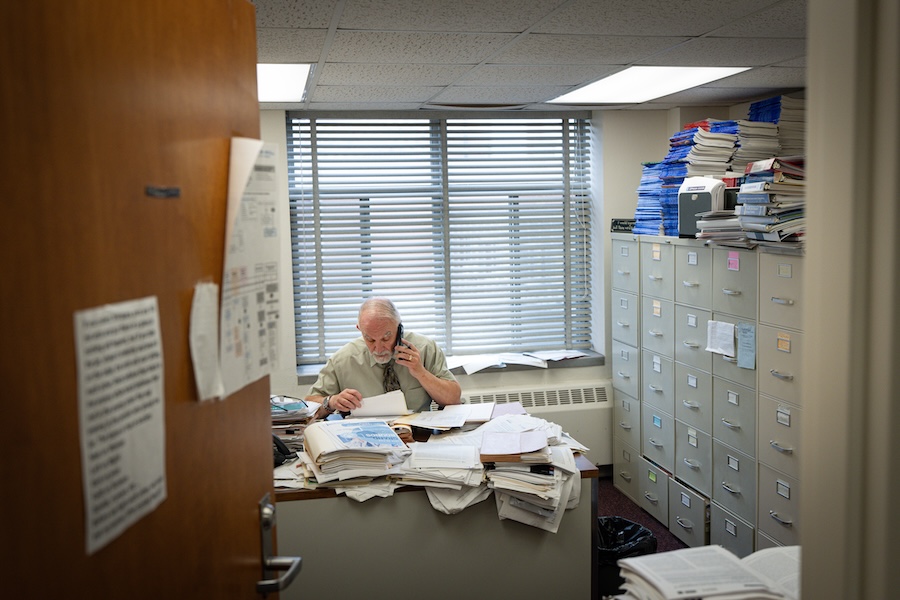
The lone physician in the clinic, Gulick received minimal help from a registered nurse and a few medical assistants. Funding was never guaranteed. Budget cuts caused the hospital to stop supporting the clinic. Gulick secured funding from Michigan State University, but only for one year. There were times, he said, when he paid the clinic’s expenses and staff from the paycheck he earned through the university and hospital.
Three decades later, Gulick still remembers the people he treated and the seemingly insurmountable challenge they faced.
He recalls one of the first patients he treated with azidothymidine, known as AZT, the first drug used to combat AIDS. Released in 1987, it slowed the disease, but the regimen created other problems for some patients.
“It had to be taken one tablet, five times a day,” he said. “You had to put your alarm clock on because you couldn’t miss a dose and you had to take it five times a day at the same time, and that’s what he did. But he continued to degenerate, and his degeneration was entirely neurologic. He developed severe AIDS dementia.
“It affected his brain and in the final days of his life, he was in a hospital bed with the side rails up so he couldn’t climb out. I caught him one time drinking his own urine. He just had no idea who he was or where he was. It was so sad; he was a brilliant [man] prior to that.”
The work took its toll on Gulick. In those early years, he said the mortality rate was 100%, and he became depressed. Looking back, he wonders if he should have sought psychological help. When he arrived at the hospital, he said his patients’ rooms looked like a murder scene, with yellow warning signs covering the doors and labels identifying the rooms as “highly contagious” and “infectious.”
In 1990, funding became available through the Ryan White HIV/AIDS Program, named after Indiana teenager Ryan White, who contracted HIV through a blood transfusion.
Dean Sienko was the health officer and medical director of the Ingham County Health Department at the time, and Gulick credits both him and Ryan White funding with keeping the clinic afloat.
Stigma against AIDS patients was rampant, even among medical professionals. Consequently, many doctors wouldn’t work with those suffering from the illness.
“I remember attending multiple conferences trying to inform medical practitioners about the true risks,” Sienko said. “There were a lot of rumors, a lot of bad information that was floating around, and I felt it was important in my role as a public health professional to inform the clinical community about what the true risks were of acquiring HIV from treating patients, and the risk was actually very low. Other than puncturing yourself with a needle, there was not any risk.
“There was a lot of fear in those days, and you can understand why people would have been nervous about it. But we hoped that with education and over time, people would understand what the risks were.”
Gulick remembered encounters with colleagues who demonstrated willful ignorance. Patients would sometimes bake him cookies or cakes to thank him, and he would share the treats in the nurses’ station.
“This individual came in and he always sampled the food and cookies left out,” Gulick said. “He said this cake I shared was really good [and] asked where it came from. I said one of my patients made it. He went into the bathroom and spit it out and got all nervous and asked me why I didn’t tell him. What was I going to tell him? He asked what he should do now and I thought, ‘He couldn’t be this stupid, could he?'”
Gulick cared for his patients not just as a dogged physician committed to their survival, but as a friend devoted to holding their hand through a disease shrouded in stigma, Sienko said
“He was just an incredible asset to our community,” Sienko said, “and particularly caring for people who had diseases that were complicated, and people who at times were neglected and not treated fairly.”
Sienko remembered after a drug was created to effectively cure hepatitis C, another disease Gulick devoted considerable effort to. Gulick ran up to Sienko, nearly shouting the good news that would save the lives of several of his patients.
“You could just see the joy in his face and in his emotions that now he could go to his patients and tell them he could cure them. He’s just a remarkable man. I have the fondest memories of him and the utmost respect for his compassion as a physician. Just an outstanding leader, mentor and example.”
Slowly, progress was made. The medical community discovered how AIDS was transmitted, how HIV caused AIDS, and in 1994, Gulick said they could begin measuring viral loads. In the mid-1990s, HAART, or highly active antiretroviral therapy, was developed as a combination of daily medications to manage HIV.
Gulick called the treatment lifesaving but expensive and complicated. Some patients needed to take 30 pills a day, each carrying a range of side effects. He went to bat for his patients, working with state officials to explain why these drugs and laboratory tests had to be covered for those without insurance.
“I had to explain in dollars and cents: would you rather have an HIV patient get AIDS and go in the hospital and cost the whole country and the state and everything else hundreds of thousands of dollars, or give them a drug so they could get back their immune system and be functional in the community and not have to spend all this money on all this kind of stuff,” he said.
Gulick met with members of Congress, senators and anyone he could think of with influence, advocating for programs such as the AIDS Drug Assistance Program, or ADAP, which he explained provides grants for HIV patients who have no insurance and are sometimes homeless. To this day, funds support basic laboratory tests and medications.
Those funds saved lives, Gulick said, especially in the early days when some of his patients had nothing.
“Many of them were just thrown out of their house,” he said. “Their families totally just ostracized them, and they were left alone. And then I had trouble getting any kind of care for them, other than the care I was giving them medically. And then psychologically, they were destroyed, devastated.”
This is where the Lansing Area AIDS Network, or LAAN, came in. Through federal grants and Ryan White funding, Gulick said it provided social workers, case managers, mental health treatment and even legal support for people living with HIV/AIDS.
Suellen Hozman was a founder of LAAN and an Ingham County registered nurse who collaborated with Gulick during the 1980s and ’90s.
“There were several areas that we tried to work in,” she said, “and one was if you had an individual with a diagnosis and they didn’t have funds, we would try to get food for them, and that was us connecting with local organizations. I mean, we didn’t have a food bank, we didn’t even have a place to meet; the first meetings were at my house.”
She said one of the most meaningful things LAAN did during those years was its buddy system, developed with local activist Doak Bloss. It paired people living with HIV/AIDS with someone who did not pass judgment and could provide companionship when they had no one else.
Hozman said she witnessed firsthand how Gulick cared for his patients.
“He was one of these unusual people,” she said, “who knows the world is made up of us, and there is no us or them, just us. There was no judgment involved, and when Peter would be with patients, he would want to know what their goals were. And for most of them, it was becoming less infectious, and in the very beginning, they just wanted to live longer because so many of them were young people, and now I would think the goal would be to be antigen negative.”
Dawk Hawk was one of Gulick’s patients. In 1991, he delivered the shattering news that she was HIV-positive and had been infected by her husband.
“I found out July 18, 1991, as a direct result of [her husband] being in the hospital,” she said. “He had been in the hospital on and off for two months. At the time, they called Dr. Gulick because they couldn’t figure out what was wrong with him. Although he kept asking to be tested for HIV, nobody listened to him. He finally demanded it because they kept saying, ‘You don’t fit the profile. You’re a white married male.’
“Back in that time, it was strictly considered a gay disease. So they tested him. When it came back positive, they waited until I was there to tell him. Apparently, the look on my face, they felt so sorry for me because I didn’t know anything.”
Hawk’s husband had been unfaithful.
She said Gulick waited in the hallway for her and told her to go directly to the lab downstairs for bloodwork to determine whether she was HIV-positive as well. She waited three weeks for the results. Gulick telephoned her with the news.
She tested positive.
“He proceeded to stay on the phone with me for 45 minutes, talking to me, making certain I was going to be all right, telling me the things I needed to do,” she remembers. “At that time, he said, ‘Be very, very careful with whom you tell.’ He said I probably should get counseling. They wanted to start me on a drug regimen. He set up an appointment with me.”
Hawk said she asked how long she would live, but Gulick told her he didn’t have a crystal ball. She didn’t think she would live very long. She connected with others who had the disease and watched as they died.
But 35 years and countless treatments and drug regimens later, Hawk is still here. She began accompanying Gulick to community seminars and presentations about HIV/AIDS, helping educate the public. Together, they spoke to churches and medical audiences alike, helping listeners see the humanity behind the diagnosis.
“One of the biggest things Dr. Gulick taught me was that I’m a person first, not a diagnosis,” she said. “That has always meant a lot to me. I think that’s one of the reasons I’ve stayed with him all these years. He has always treated me like a person, not like a disease.
“When I was first diagnosed, I was planning my funeral. Now I’m planning for retirement. I never imagined I’d get old.”
With today’s treatments, Gulick said the life expectancy of his patients can be within three to four years of someone who does not have HIV. He said he has an 86-year-old patient with HIV, and as long as patients take their medication, they can expect to live lives that once seemed unimaginable.
The goal today is what Gulick describes as “U equals U,” or undetectable equals untransmittable. With today’s medications, patients can achieve an undetectable viral load, making the virus untransmittable.
In 2006, a once-daily pill regimen was developed, and treatments have only become more effective and simpler. Today, Gulick said Cabenuva injections are a common treatment, sometimes administered only every other month.
Kristina Schmidgall is LAAN’s director. She began as a volunteer in 2000, working at the front desk and helping with HIV testing.
She spoke about the impact Gulick continues to have on patients, particularly those who are newly diagnosed, helping them understand that HIV is no longer a death sentence. She said he goes the extra mile for people with unstable housing or employment, recognizing that those challenges affect their care.
“I feel like Dr. Gulick isn’t just like, ‘I only do HIV,'” she said. “He’s like, ‘Okay, are you seeing a case manager? If not, can we get you some services? How can we do this?’ Realizing that it’s the whole person and not just a matter of, ‘Are you taking your medications?’ because those other things impact that.
“I’ve known some HIV doctors who have been really like, ‘What’s the point of case management?’ Not looking at people and our clients as a whole, because our clients are more than the HIV diagnosis and more than the medications they take. There’s so much more going on.”
Gulick said his patients, including many he has treated for decades, will sometimes ask if he plans to retire.
“As long as I feel good and I can still think clearly,” Gulick said, “I’m going to be here until a cure comes about. And I’m always hoping that maybe I can see the last chapter before I do retire.
“I never thought we’d get to this point, to be honest with you. If you were to tell me back in the late ’80s or even early ’90s that we’d be at this point now, I’d think you were nuts.”